Dillon, Lucy (2016) Community mobilisation and local alcohol action plans: an evaluation. Drugnet Ireland, Issue 58, Summer 2016, pp. 27-28.
| Preview | Title | Contact |
|---|---|---|
|
PDF (Drugnet 58)
745kB |
A report on the National Community Action on Alcohol Pilot Project (NCAAPP) was published in December 2015.1 The findings of this report, a process evaluation of the project which began in 2015, are outlined below.
Background
On foot of the National Substance Misuse Strategy,2 the remit of the drugs task forces was expanded in 2014 to include alcohol. To support the task forces in meeting the demands of this new remit, the NCAAPP was established. Its aim was to support task forces in developing a ‘community mobilisation approach’ which would inform the development of policies to address alcohol use, and reduce alcohol-related harm, in their area. The project was delivered by the Alcohol Forum in partnership with the Drug Programmes and Policy Unit of the Department of Health and the Wellbeing Division of the Health Service Executive.
Community mobilisation
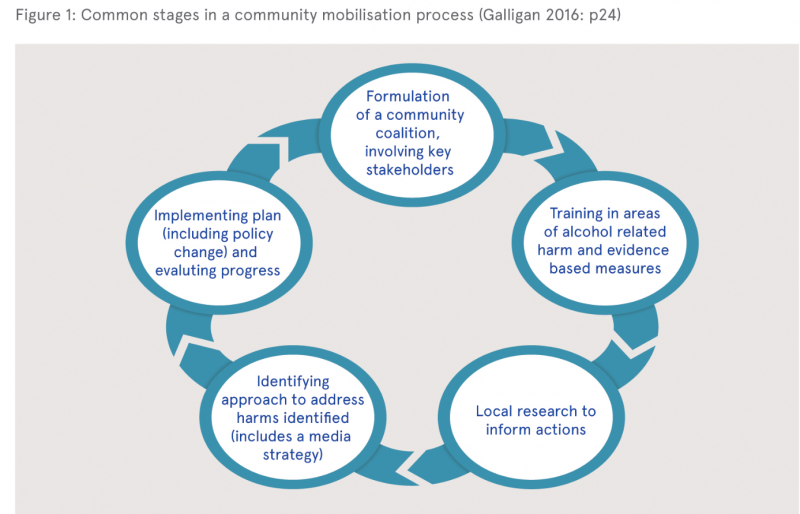
Underpinning the pilot project’s approach was the finding of the National Substance Misuse Strategy that community mobilisation is successful in bringing stakeholders together to develop alcohol and drug policies. The author of the evaluation report describes community mobilisation as a public health approach to reducing alcohol-related harm: it changes the context in which alcohol use occurs, rather than focusing on the ‘problem drinker’. It is a process through which communities work together to take action and bring about change, working with a range of stakeholders from the public, statutory and private sectors to identify the changes they want to bring about in their area. Based on the best evidence available the different stakeholders plan together how to bring about the desired changes. The community then implements the plan and monitors its progress in reducing alcohol-related harm. Some common features of the approach are shown in Figure 1.
The evaluation report contains a review of the literature on community mobilisation and shows how elsewhere it has been effective in reducing alcohol-related harm. The author identifies key elements that contribute to positive results when working in this way, including:
- establishing well-functioning coalitions,
- getting wider community buy-in to the process and its aims,
- changing the policy context,
- taking an evidence-based approach,
- giving the project adequate time to get established and deliver on outcomes (in excess of three years),
- taking a multi-strategy approach, and
- using the media to support interventions.
Evaluation findings
Drawing any conclusions about the effectiveness of the NCAAPP in reducing alcohol-related harm was beyond the scope of this evaluation. Instead, the report explored the effectiveness of the process put in place to deliver on community mobilisation and to establish local alcohol action plans.
Five task forces were selected to take part in the project, each of which identified a project lead and established an ‘alcohol sub-committee’ with responsibility for delivering on the project in their area. Each sub-committee sent a representative on five one-day formal training sessions in Dublin. These covered a range of topics including community mobilisation, data collection, research and evaluation methods, logic models, alcohol-related harm, using the media, and effective policy measures to address alcohol harms. The task forces then received on-site tailored support to help develop their local plans, as well as access to follow-up support via phone calls, emails, one-on-one meetings and some on-site group training. One individual from the Alcohol Forum had responsibility for delivering this programme of training and support.
Broadly speaking, the goals of the project were to train stakeholders on drug-related harm, raise awareness of policy measures, support community engagement, and develop local action plans. The evaluation found that, overall, the project was successful in these areas.
The training and support delivered was of a high quality and was delivered by a highly dedicated trainer. Participants improved their knowledge of alcohol-related harms and the networking opportunities afforded by the centralised training sessions were seen as beneficial. The training also led to changes in work practices, for example a public health approach to alcohol issues was adopted, evidence-based measures were applied, and a community mobilisation model was used.
At the core of the project was the production of local alcohol action plans. Four of the five task forces completed local alcohol action plans by the end of the project and the fifth had an outline plan. All the completed action plans included monitoring, review and self-evaluation measures.
A number of critical barriers were identified. Building local leadership and commitment to the project proved challenging, as did engaging stakeholders to lead a collective approach. Limited resources presented hurdles when it came to making and implementing a plan. Finally, local policy changes to help lower alcohol-related harm needed to be reinforced by a government-level commitment to adopting such evidence-based policies.
The author made a range of recommendations at the end of the report. She highlighted the fact that community action on alcohol is a long-term process and that the pilot project was just the beginning of the process for those involved.
1 Galligan C (2016) National community action on alcohol pilot project 2015: external evaluation project. Dublin: Department of Health https://www.drugsandalcohol.ie/25098/
2 Department of Health (2012) Steering group report on a national substance misuse strategy. Dublin: Department of Health. https://www.drugsandalcohol.ie/16908/
B Substances > Alcohol
J Health care, prevention, harm reduction and treatment > Risk and needs assessment > Needs assessment > Community needs assessment
L Social psychology and related concepts > Participation / involvement / engagement / co-production
MA-ML Social science, culture and community > Community action > Community development
MA-ML Social science, culture and community > Community action > Community involvement
VA Geographic area > Europe > Ireland
Repository Staff Only: item control page