Lyons, Suzi (2016) On and off methadone substitution treatment: risks of mortality. Drugnet Ireland, Issue 57, Spring 2016, pp. 6-8.
| Preview | Title | Contact |
|---|---|---|
|
PDF (Drugnet 57)
1MB |
A recently published study aimed to assess the risk of death when initiating or stopping methadone treatment in primary care.1 In addition, the study led to assess the effect of supervised methadone consumption on mortality rates.
Data from the Central Treatment List (CTL) were used to identify cases that were in receipt of at least one methadone prescription in primary care over the six years between August 2004 and December 2010. The CTL data were linked to the Methadone Treatment Scheme (MTS) dispensing records. These were further linked to the General Medical Services (GMS), which contains information on all other prescription medication, excluding methadone. Finally, these were linked to the mortality data recorded by the National Drug-Related Deaths Index (NDRDI). A case was considered ‘off treatment’ if the individual had not received a new methadone prescription for three days since the end of their last prescription. They were considered ‘off treatment’ until a new prescription was generated.
The main outcome measure was drug-related mortality, defined as a death due to poisoning as per the NDRDI definition. The second outcome measure was all-cause mortality.
In total, 6,983 cases aged between 16 and 65 years who received methadone were included in the study. Of these, the majority were male (69%) and 57 per cent were aged 29 years or younger (Table 1). The majority of cases had received methadone treatment five or more times, with a treatment period lasting a median of 83 days. Three per cent (n=213) of those included in the study died during the study period.
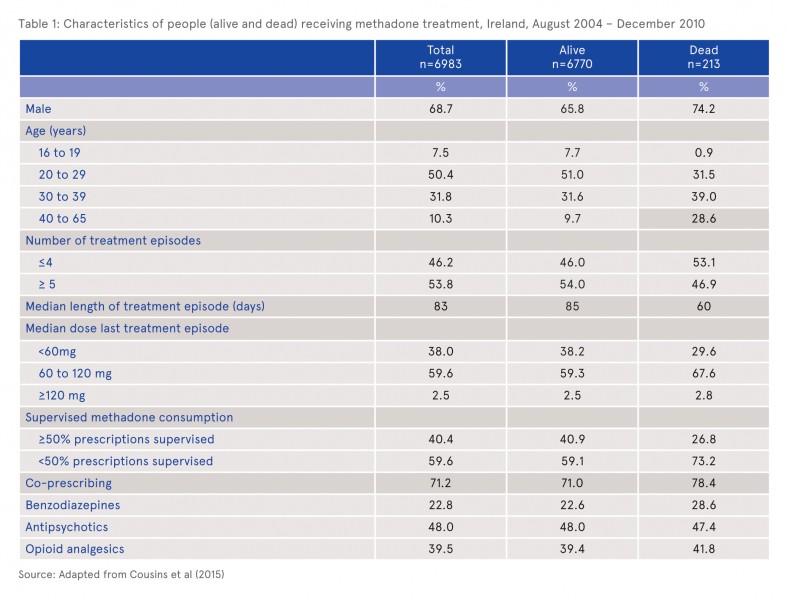
Of the 213 people who died, 98 (46.0%) were classified as being off methadone treatment. The deaths of over a third (78, 37%) were classified as being due to poisoning. Opiates (n=72) and benzodiazepines (n=56) were the drugs most frequently reported in the toxicology reports on these cases. The risk of dying because of poisoning was highest when a person was off treatment (0.39 deaths per person years) compared to on treatment (0.24 per person years) but this was not statistically significant. For those off treatment, mortality rates from poisoning were highest in weeks one to two (0.49 deaths per person years) and in weeks three to four (1.19 deaths per person years). Again, there was no statistical difference between the time periods or from those on treatment.
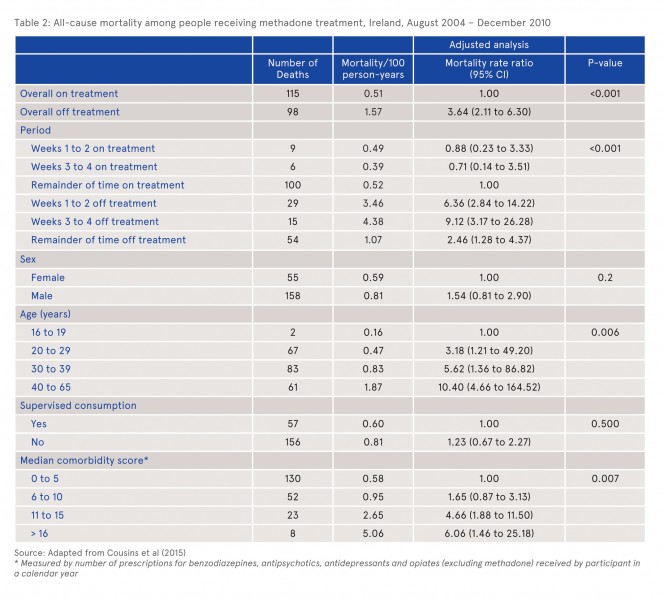
Analysis of all-cause mortality, adjusted for gender, age and comorbidity, showed that people who were off treatment were three times more likely to die than those on treatment (3.6, 95% CI 2.1 to 6.3) (Table 2). The risk of mortality was highest in the third and fourth week after stopping treatment (9.1, 95% CI 3.1 to 26.2). However, the risk of mortality off treatment after five weeks or more remained higher than being on treatment. A higher risk of dying was associated with age and increased co-morbidity, as shown by the median co-morbidity score. The authors noted that in the unadjusted analysis, mortality was higher among those whose methadone consumption was not supervised (1.36, 95% CI 1.00 to 1.84) but this was not found to be statistically significant in the adjusted analysis.
One of the potential limitations of the study was the definition of ‘off treatment’ as not receiving a methadone prescription for three days since the end of the last prescription. This cut-off was based on UK guidelines which are based on reduction of tolerance. However, a sensitivity analysis extending the cut-off to seven days also showed increased mortality off treatment, 3.06 (95% CI 1.74 to 5.39). Another limitation was that people transferring from primary care to specialist methadone clinics were not included and so were classified as ‘off treatment’. These limitations were compounded by the lack of information on those who were off treatment, for example they may have been in prison, had stopped their opiate use or have been hospitalised.
While acknowledging the strengths of the study, such as the large national cohort of people receiving methadone who were included and the detailed prescription data from primary care, the inability to control for the residual confounders noted above is often a problem in such observational studies and the findings from this study should be viewed as a basis for further research. In particular, the authors recommended further research in relation to supervised consumption.
The findings also have implications for national practice and policy as it shows that retention in treatment in primary care is associated with a reduced risk of all-cause mortality. The authors also recommended that when a person leaves methadone treatment in primary care there should be improved post-treatment monitoring and follow-up for the first month, when relapse rates are highest along with the greatest risk of dying.
Editorial comment
In response to this newly-published Irish study on the risks of mortality on and off methadone substitution treatment in primary care, Professors Matthew Hickman, John MacLeod and Louisa Degenhardt wrote an editorial in the journal Addiction, stating: 2
The National Irish cohort study strengthens evidence on the hazards of leaving opioid substitution treatment (OST) and the dangers of short duration treatment and provides the first piece of evidence for future synthesis of the effect of supervised consumption on mortality risk in people on OST.
In their commentary, they stressed the need for robust and reliable evidence to enable service providers to provide the best possible drug treatment in order to reduce mortality in this vulnerable cohort of people. This evidence is particularly pertinent when wanting to understand if changes in drug treatment have had any impact on mortality or outcomes. The professors also noted that this Irish study had provided some weak evidence suggesting that supervised consumption may reduce the risk of mortality but further evidence is needed to build on this finding.
- Cousins G, Boland F, Courtney B, Barry J, Lyons S and Fahey T (2015) Risk of mortality on and off methadone substitution treatment in primary care: a national cohort study. Addiction 111 (1): 73-82. https://www.drugsandalcohol.ie/24374/
- Hickman M, Macleod J and Degenhardt L (2016) Commentary on Cousins et al (2016): Accumulating evidence on risk of mortality on and off opioid substitution treatment. Addiction (111): 83–84.
B Substances > Opioids (opiates) > Opioid product > Methadone
F Concepts in psychology > Behaviour > Risk-taking behaviour (delay discounting)
HJ Treatment or recovery method > Substance disorder treatment method > Substance replacement method (substitution) > Opioid agonist treatment (methadone maintenance / buprenorphine)
J Health care, prevention, harm reduction and treatment > Risk and protective factors > Risk factors
P Demography, epidemiology, and history > Population dynamics / statistics > Substance related mortality / death
VA Geographic area > Europe > Ireland
Repository Staff Only: item control page