Dillon, Lucy (2022) Focused policy assessment of the national drugs strategy. Drugnet Ireland, Issue 80, Winter 2022, pp. 8-12.
| Preview | Title | Contact |
|---|---|---|
|
PDF (Drugnet Ireland 80)
1MB |
On 13 August 2021, as part of the 2021 Government spending review process, the Focused policy assessment of Reducing Harm, Supporting Recovery: an analysis of expenditure and performance in the area of drug and alcohol misuse was published.1 This focused policy assessment (FPA) of the national drugs strategy2 was prepared by staff of the Irish Government Economic and Evaluation Service (IGEES) based jointly in the Department of Health and the Department of Public Expenditure and Reform.
Aim of the focused policy assessment
The purpose of FPAs by the IGEES is to set out the rationale for a particular policy intervention; the public resources provided to support its delivery; the related outputs and services that are provided; and the achievements of the intervention relative to its stated goals. There are two main elements to the current review:
- Drug-related public expenditure (labelled and unlabelled): The review profiles labelled expenditure and presents the findings of the first effort to estimate unlabelled expenditure in an Irish context. This estimate is based on medical and judicial costs as well as lost productivity.
- Reducing Harm, Supporting Recovery (RHSR) performance against its performance indicators (PIs): The review maps the availability of data for the strategy’s 29 PIs and analyses those that are available (for 12 PIs), in an attempt to assess the performance of RHSR under its five strategic goals.
The authors focused on the timeframe 2014–2020 in order that data could be analysed for comparison before and after the implementation of RHSR in 2017.
Drug-related public expenditure
Labelled public expenditure
Labelled drug-related expenditure is defined by the European Monitoring Centre for Drugs and Drug Addiction (EMCDDA) as ‘the ex-ante planned public expenditure made by general government in the budget that reflects the public and voluntary commitment of a country in the field of drugs. In addition, it is any expenditure identified as drug-related in public accountancy documents’3 (p. 23). In Ireland, it includes budget allocations for the Health Service Executive (HSE) Addiction Services and treatment services in prisons, for example. The authors report the expenditure data as they appear in Ireland’s 2020 National Report for the EMCDDA4 (see Table 1).
The authors note that while total expenditure appears to have decreased since 2016, this in fact reflects limitations in data reporting. Based on the available data, the largest increase in organisational spend over the period 2014–2019 was by the HSE Addiction Services – an increase of €17 million, an average year-on-year increase of 4% per annum.
Unlabelled public expenditure
A core part of the FPA is the work that went into developing an estimate of unlabelled expenditure on drug use in Ireland. Unlabelled drug-related expenditure is the ‘non-planned or non-publicly announced ex-post public expenditure incurred by the general government in tackling drugs that is not identified as drug-related in the budget’ (p. 24).3 This would include, for example, the cost incurred for the imprisonment
of people for drug-related offences.
While Irish estimates have been made for alcohol use,5,6,7 they have not been made for other drugs. The authors argued that this presented ‘an obstacle to assessing the cost-effectiveness of publicly funded interventions, since any examination of the value of measures to alleviate the clinical, social and environmental harms of illegal drugs ought to relate changes in inputs (planned programmes to tackle this issue) to changes in outputs and costs’ (p. 20).1
Table 1: Public expenditure directly attributable to drug programmes (labelled), 2014–2019
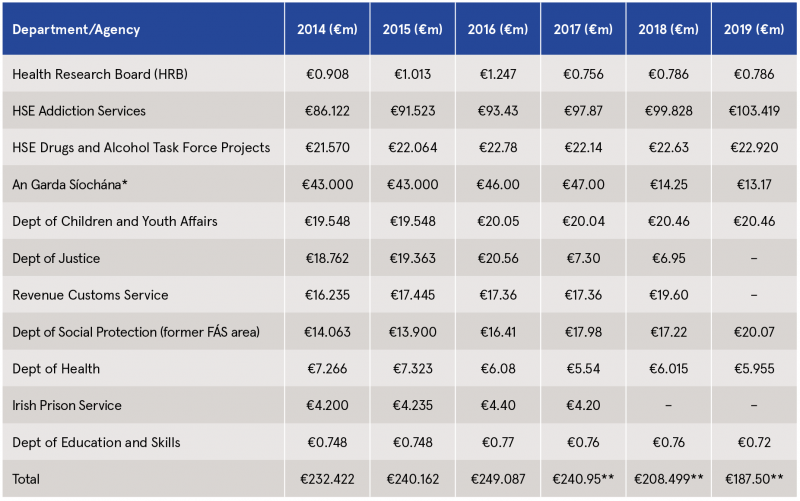
Source: Health Research Board (2021)4
* After 2017, An Garda Síochána moved from reporting on ‘policing/investigation costs’ to ‘policing/investigation costs of Garda National Drugs and Organised Crime’ only.
** The €53m decrease in expenditure between 2017 and 2019 reflects limitations in reporting of expenditure from An Garda Síochána, Department of Justice and Equality, Irish Prison Service, and Revenue Customs Service, rather than a reduction in expenditure as such.
Methodological approach
To develop the estimate, the authors focused on drug-related costs in prisons and acute hospitals. The selection was based on the assumption that they would account for a relatively large proportion of unlabelled expenditure. In addition, they examined a selection of economic costs (productivity losses associated with hospital treatment and imprisonment) and societal costs (premature drug-related death).
The review estimates unlabelled costs using both cross-sectional and longitudinal approaches. However, for the purpose of this summary, the focus is on the former, as it examines costs on an annual basis and therefore relates to the annual budgetary cycle as per labelled expenditure. The approach taken for each area of interest is described here in its simplest terms.
- Prison and criminal justice costs: Costs related to drug offences (importation, manufacture or possession) and drug-related crime were examined. Identifying drug-related crime presented methodological challenges as it required estimating the causal link between drug use and other types of crime, i.e. what proportion of crimes such as theft or public order offences can be attributed to drugs and therefore be defined as drug-related crime? To address this challenge, the authors adopted a framework of drug attribution fractions (DAFs) developed in the United States, and which estimate the proportion of different types of crime that are attributable to illicit drug use.8 DAFs were combined with information about the duration of sentences for people imprisoned for drug-related offences and controlled drug offences. An estimate of average costs per offence as well as a range of other parameters were used to provide an estimate of drug-related crime costs.
- Healthcare costs: Acute hospital costs were estimated for admissions directly related to drug use, as well as admissions for health problems associated with drug use. DAFs were also used as part of the model, which included parameters on healthcare resource use and costs for the various conditions.
- Productivity losses: Time spent in prison or hospital and premature death due to drug misuse represent a loss in economic output. The authors took a ‘human capital approach’ (p. 25)1 in an effort to assess the costs involved. They estimated the costs of displaced paid labour, using median annual earnings and employment rates by age and gender, and analysed this with the relevant data source for prisons, acute hospitals, and premature deaths.
Results
Table 2 provides the estimates of the unlabelled costs associated with problem drug use under each of the four headings examined through cross-sectional analysis. (Note that the findings of the longitudinal analysis can be found on page 27 of the review.) The annual direct costs of hospital treatment, criminal offences, and prison committals for a cohort of affected individuals in Ireland is estimated to be approximately €87 million, and when indirect productivity costs are included (mainly as a result of premature deaths) this rises to over €147 million.
Table 2: Estimates of annual unlabelled drug-related expenditure, based on cross-sectional analysis

Limitations
Limitations to these estimates are covered in detail in the review. They relate to the data available to conduct the analysis as well as a recognition that there is a range of other methodological approaches that if utilised would have produced different estimates. However, the authors argue that the aim of their analysis ‘was to characterise, rather than precisely estimate, the different types of unlabelled expenditure and productivity costs associated with problem drug use’ (p. 27).1
Concluding comment on expenditure analysis
The data available on drug-related public expenditure are limited. However, the findings suggest that the unlabelled costs ‘contribute significantly’ to the overall economic burden of problem drug use and are therefore an ‘important component of any policy-orientated analysis of the marginal costs and effects of changes to the provision of addiction and treatment services’ (p. 27).1 The same message is true for labelled expenditure.
Performance indicator analysis
The FPA aimed to assess the performance of RHSR by analysing the data available for the PIs under each of its five strategic goals. There were three phases to this work: data scoping, collection, and analysis. Data scoping found that there were significant limitations in the availability of data. The reasons for this included that the data did not exist, it could not be accessed, or did not fit an appropriate timeframe. Where possible, proxy data were used but overall data were found for only 12 of the 29 PIs. Data were provided by the Health Research Board (HRB), HSE, Revenue, An Garda Síochána, Central Statistics Office (CSO), and the European School Survey Project on Alcohol and Other Drugs (ESPAD) and Health Behaviour in School-aged Children (HBSC) surveys. Data were collated and charts created using Excel software, which facilitated a trend analysis of each indicator where possible.
Results
Despite the limitations, some of the key findings under each strategic goal identified in the discussion of the review are noted here.
Goal 1: Promote and protect health and wellbeing
Available data for this goal focus on rates of substance use among children and young people. The findings would suggest that young people’s drug use is reducing or ‘holding steady’ (p. 68). Nevertheless, the authors identify heavy episodic drinking among 15–16-year-olds as being of concern. They flag the Drug Prevalence Survey as an important source of information for this goal.9 However, the latest wave of the survey had not been published at the time the review was written.
Goal 2: Minimise the harms caused by the use and misuse of substances and promote rehabilitation and recovery
The review draws extensively on data from the National Drug Treatment Reporting System (NDTRS) for this goal. Key findings included:
- Since December 2018, over 90% of problematic substance users had accessed treatment in NDTRS services within a month of assessment for those aged 18 and over, and a week for those under the age of 18. This measure does not include the numbers of people waiting for assessment.
- ‘Successful exits’ from treatment averaged at 47% from 2014 to 2019, although there was variation across different substance and treatment types.
- The median number of years between starting to use drugs and entering treatment (lag) for those cases recording a successful exit dropped from 20 to 17 years in 2018, and remained at 17 years in 2019. This lag to treatment time may vary significantly by treatment type.
- Access to opiate substitution treatment (OST) rose steadily between 2014 and 2020. In 2014, the number in receipt of OST was approximately 9,300, rising to 9,974 by the end of 2019; in June 2020, it was 10,465. This latest increase can in part be explained by the services’ response to the Covid-19 pandemic.
There is a gap in knowledge about problematic substance users who are not in contact with services. The authors argue that ‘understanding the unmet need for services is important in interpreting much of the results under Goal 2 and as such the conclusions that can be drawn are constrained by this’ (p. 69).1
Goal 3: Address the harms of drug markets and reduce access to drugs for harmful use
Key findings in relation to drug markets and access to drugs include:
- There was a downward trend in the number of recorded offences for cultivation or manufacture of drugs from 345 in 2014 to 192 in 2019.10
- The trend for offences for importation of drugs has remained relatively stable over the period 2014–2019.10
- Possession offences (possession for sale and supply and possession for personal use) have been increasing since 2015.10
- There has been an increase in the quantity (kg) of drugs seized in recent years, while the number of seizures has increased since 2017.
- Rates of driving while over the legal alcohol limit have reduced since 2017. However, the number of offences for driving while under the influence of drugs has risen over the same period. This is likely, at least in part, to be linked to changes in the testing system.10
Goal 4: Support participation of individuals, families, and communities
Due to poor availability of data, the only measure reported under Goal 4 was the uptake of treatment by members of the Irish Travelling, LGBTQI, and homeless communities. According to NDTRS data, members of the Travelling community increasingly do not take up treatment after being assessed (from 6% in 2014 to 10% in 2019); a similar trend was found among people who are homeless. Uptake of treatment for cases of individuals who are homosexual and bisexual has remained stable over the period.
Goal 5: Develop sound and comprehensive evidence-informed policies and actions
The only data to be analysed under Goal 5 came from the NDTRS. Between 2014 and 2019, there has been a small increase in the number of services providing treatment; however, the number who submit data to the NDTRS has been consistent at approximately 600 over the period.
Concluding comment on PI analysis
Similar to the expenditure analysis, the overarching message from the analysis of the PIs was that ‘limitations in the availability of data has constrained the conclusions that can be drawn on the progress made under each goal, and in turn the overall performance of RHSR’ (p. 70).1 The authors also raised the question of attribution. Drug use and its causes are complex; therefore, any changes found are not necessarily attributable to RHSR.
Overall conclusions
The authors also draw conclusions based on their findings. These include:
- The available evidence base on the costs of drug and alcohol misuse is limited by data availability and is estimated using varied methodological approaches. There is a need to improve the reporting of labelled expenditure across Government Departments and to gain consensus about the best approach to estimating unlabelled expenditure in this area. The authors suggest that there is a need to unpack the expenditure data in a more systematic way to fully understand its limitations.
- The findings indicate that ‘unlabelled expenditure and productivity costs contribute significantly to the overall economic burden of problem drug and alcohol use’ (p. 6).1 Therefore, it is an important element of any analysis to look at the value of policies in this field in terms of changes that may be brought about.
- Limitations in the availability and quality of data on the PIs have constrained the conclusions that could be drawn on the performance of the strategy. While some data will become available in the next phase of the strategy, in some cases PIs will need to be revised in order to more accurately reflect performance under that goal.
- The proportion of labelled expenditure could not be broken down by either that spent on health-led responses as opposed to criminal-led responses, or by strategic goal of RHSR. In addition, the limitations in the detail and quality of expenditure data (labelled and unlabelled) meant that the authors were unable to make an assessment of what had been achieved for expenditure to date by RHSR. The authors argue that addressing the limitations of the datasets are necessary steps for improved monitoring and future evaluation of RHSR and public expenditure on drug and alcohol programmes more generally.
Despite its limitations, this review represents a valuable step towards generating the economic evidence base upon which public policy on drug use can be evaluated. Overall, it highlights the need to improve the data collection process, to adopt PIs that are measurable for the remainder of the strategy’s lifetime, and to agree the optimal methodological approach to analysing expenditure and PI-related data.
1 Bruton L, Gibney S, Hynes T, Collins D and Moran P (2021) Spending review 2021. Focused policy assessment of Reducing Harm, Supporting Recovery: an analysis of expenditure and performance in the area of drug and alcohol misuse. Dublin: Government of Ireland. https://www.drugsandalcohol.ie/34729/
2 Department of Health (2017) Reducing Harm, Supporting Recovery: a health-led response to drug and alcohol use in Ireland 2017–2025. Dublin: Department of Health. https://www.drugsandalcohol.ie/27603/
3 Bretteville-Jensen AL, Costa Storti C, Kattau T, Mikulic S, Trigueiros F, Papamalis F, et al. (EMCDDA) (2017) Public expenditure on supply reduction policies. Brussels: Council of Europe. http://www.drugsandalcohol.ie/27458/
4 Health Research Board (2021) Focal Point Ireland: national report for 2021 – drug policy. Dublin: Health Research Board. https://www.drugsandalcohol.ie/25262/
5 Mongan D and Long J (2016) Alcohol in Ireland: consumption, harm, cost and policy response. HRB Overview Series 10. Dublin: Health Research Board. https://www.drugsandalcohol.ie/25697/
6 Hope A (2014) Alcohol literature review. Dublin: Department of Health. https://www.drugsandalcohol.ie/25324
7 Byrne S (2010) Costs to society of problem alcohol use in Ireland: a report for the Health Service Executive. Dublin: Health Service Executive. https://www.drugsandalcohol.ie/15781/
8 National Drug Intelligence Center (2011) The economic impact of illicit drug use on American society. Washington DC: US Department of Justice National Drug Intelligence Center. Available online at: https://www.justice.gov/archive/ndic/pubs44/44731/44731p.pdf
9 Mongan D, Millar SR and Galvin B (2021) The 2019–20 Irish National Drug and Alcohol Survey: main findings. Dublin: Health Research Board. https://www.drugsandalcohol.ie/34287/
10 The Central Statistics Office (CSO) publishes recorded crime statistics based on the provision of PULSE data by An Garda Síochána. Data are reported quarterly. The CSO publishes these data under the category ‘under reservation’. This categorisation indicates that the quality of these statistics do not meet the standards required of official statistics published by the CSO.
MP-MR Policy, planning, economics, work and social services > Policy > Policy on substance use
MP-MR Policy, planning, economics, work and social services > Programme planning, implementation, and evaluation
MP-MR Policy, planning, economics, work and social services > Programme planning, implementation, and evaluation > Programme planning (strategy)
MP-MR Policy, planning, economics, work and social services > Economic policy
VA Geographic area > Europe > Ireland
Repository Staff Only: item control page