Assessing progress under the NDS 2001–2008, the Steering Group that drafted the new NDS found that 20 out of 22 actions to support co-ordination had been implemented, the key performance indicators relating to co-ordination reached, and that the co-ordination arrangements had ‘stimulated and promoted inter-agency working in a difficult cross-cutting policy and service area’ (para. 6.7). However, the Steering Group also found that there were ‘capacity and structural limitations’, which were limiting ability to meet the new challenges, including:
° accounting for expenditure;
° governance;
° mainstreaming;
° capacity of services to meet client needs; and
° monitoring/evaluation.
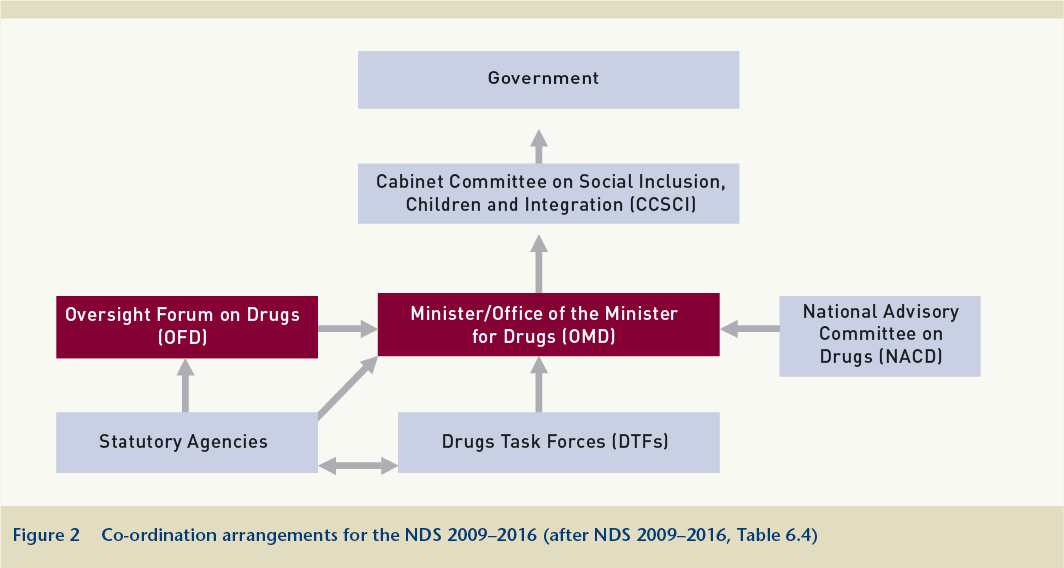
The need was identified to establish a structure which would:
° support and drive the ongoing implementation of the NDS, while respecting the various lead roles and statutory responsibilities of the Departments/agencies involved;
° provide a more cohesive and integrated framework that promotes closer co-operation and accountability between the different players, as well as greater transparency for expenditure;
° provide a clear hierarchy and a greater transparency of the roles from the government and the Cabinet Committee on Social Inclusion, Children and Integration to the local project level.
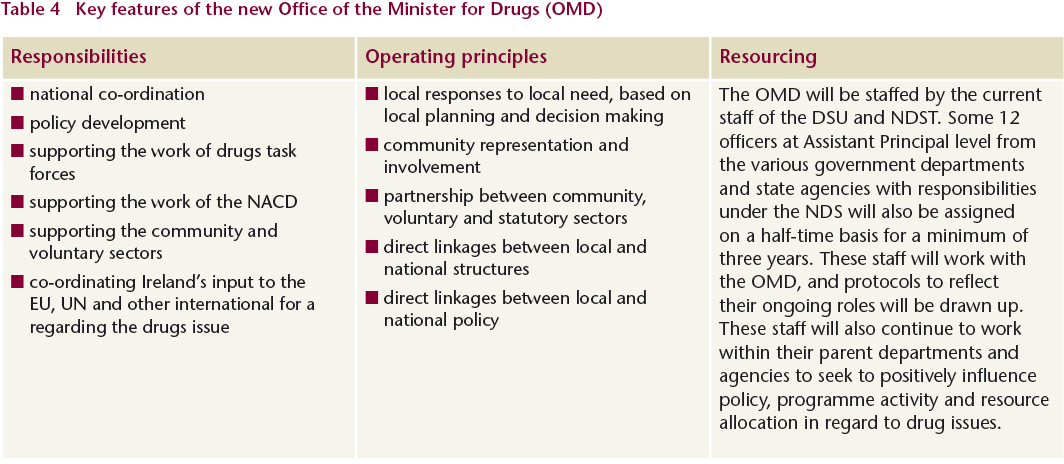
The design of the OMD resembles the networking model promoted in a recent OECD review of the Irish public sector.3 The OECD review described the Office of the Minister for Children and Youth Affairs (OMCYA), established in 2005, where staff from different government departments (including Health, Education and Justice) had been brought together in one location (the Department of Health and Children) to work in a networked way on issues of strategic national importance with regard to children. The review’s observations on the OMCYA may be applied equally to the new OMD:
Policies that cut across the function responsibility of a number of departments can lead to difficulties in determining who is the overarching ‘owner’ accountable for the service provided. The work to date by the OMC has demonstrated that there is value in ensuring that units, such as the Irish Youth Justice Services, remain connected to their parent department (Department of Justice, Equality and Law Reform). This ensures that they have ongoing interaction with, and input to the development of policies targeted at children while also ensuring that accountability for the services they deliver remains within the remit of their Minister. This guarantees that historical mismatches between children’s policy and youth justice policy can be addressed. (pp. 241–242)
To support integration, the Steering Group recommends an Oversight Forum on Drugs (OFD) to replace theInterdepartmental Group on Drugs (IDG). Comprising the same membership, its primary role will be the high-level monitoring of progress being achieved across the strategy and agreeing appropriate ways forward where issues are blocked or progress is being impeded. It will also provide a forum for discussion and feedback on issues relating to problem drug use that arise in EU and international arenas. The Group proposes two additional mechanisms to support the new integrative role of the OMD: (1) an Advisory Group of the OMD, comprising representatives of the statutory, voluntary and community sectors, to advise the Minister on operational and policy matters relating to the NDS; and (2) twice-yearly bilateral meetings between the Minister for Drugs and the ministers for Justice, Education and Health; the Minister and the Director of the OMD and the heads of various departments and state agencies involved in implementing the NDS; the Minister and the Director of the OMD and the chairs and co-ordinators of the DTFs; the Minister and the Director of the OMD and the NACD and the Family Support Network. The Steering Group believes these meetings would help to keep a focus on drug-related issues and the broader implementation of the NDS.
This multiplicity of mechanisms raises the question as to whether there is a more efficient and effective means of integrating effort across the statutory, voluntary and community sectors and engaging all stakeholders in the deliberation over and choice of policy options. For example, a study of whole-of-government approaches to cross-cutting policy issues in Ireland in the 21st century4 described how social partnership can perform such an integrating function. Advisory groups such as the National Economic and Social Council (NESC) or the National Economic and Social Forum (NESF), with broad-based representation of all the social partners and reporting to the Department of the Taoiseach, have played and continue to play a critical role in supporting the development and implementation of key national policies.5
The National Advisory Committee on Drugs (NACD) is to be co-located with the OMD and the Director of the NACD is to become a member of the senior management team in the OMD. While acknowledging the need for the NACD to be ‘independent’ in regard to research, the Steering Group states that the closer alignment with the OMD will ‘better address the issue of linkages between policy development and research’.
Local and regional drugs task forces will now report to the OMD for all activities, outputs and expenditures. Priorities for the new OMD with regard to the DTFs will include:
° considering reporting and accountability arrangements for DTF projects with a view to simplifying the system;
° examining the feasibility of achieving the optimum structure for the employment arrangements of DTF personnel;
° reviewing and renewing the commitment and participation of all members of DTFs, including the position of chairperson;
° updating the handbook for the operation of DTFs to take account of the new structural arrangements and include guidelines on mainstreaming.
The NDS notes that the National Drugs Rehabilitation Implementation Committee will also be ‘closely linked’ to the OMD.
Steering Group’s assessment of the National Drugs Strategy 2001–2008
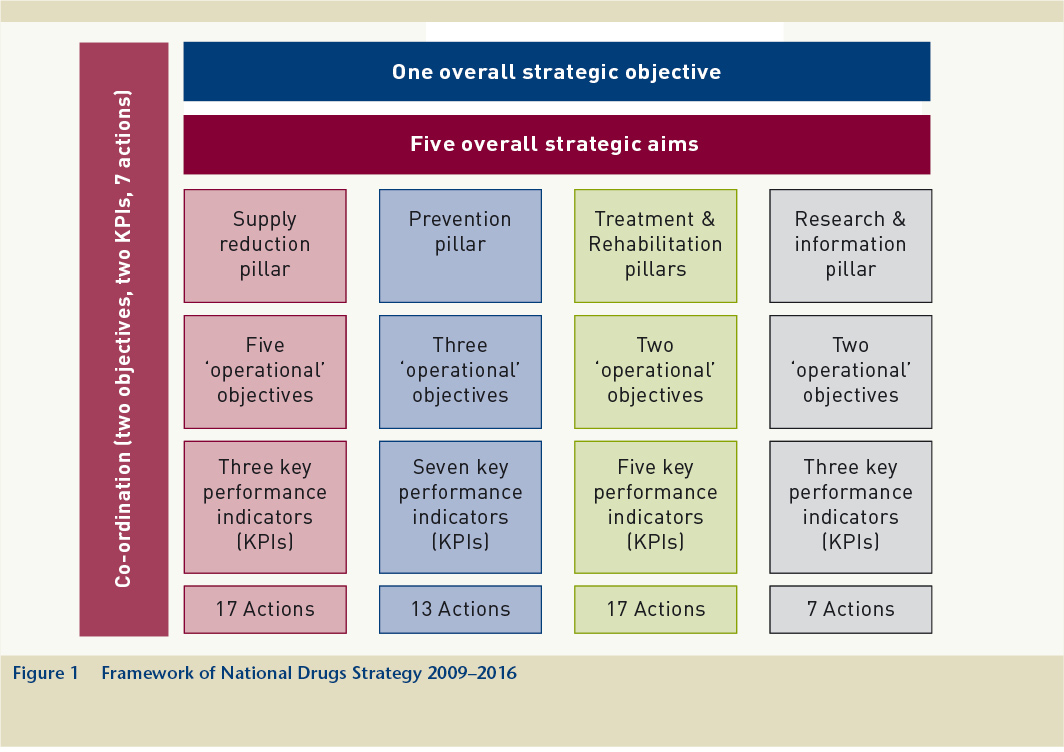
The Steering Group that managed the preparation of the NDS 2009–2016 assessed the progress that had been made against the key performance indicators (KPIs) under each of the pillars of the 2001–2008 strategy: supply reduction, prevention, treatment, rehabilitation and research.6 The Group’s assessment, as reported in the new strategy document, is summarised below.
Supply reduction
All KPIs under this pillar were achieved. The targets of a 50% increase in volume of drugs seized based on 2000 figures and a 20% increase in the number of seizures based on 2004 figures were both exceeded. The 125% increase in supply detections between 2004 and 2008 significantly exceeded the target of 20%. While acknowledging the operational success which this represented for law enforcement, the Steering Group notes that, without a reliable estimate of the size of the illegal drug market in Ireland, the impact of increased seizures on the overall supply could not be measured.
Other areas of progress included increases in the Garda Síochána resources in LDTF areas and various initiatives aimed at reducing the supply of drugs, such as the ‘Dial to Stop Drug Dealing’ scheme, undertaken by local and regional DTFs. Less progress was achieved in expanding community policing fora (CPFs) and reducing the availability of drugs in prisons.
Prevention
The KPIs under this pillar related to levels of problem drug use, prevalence, substance use policies in schools and rates of early school leaving. Heroin use stabilised in the Dublin area, with a significant drop in new entrants, but rose substantially outside Dublin. Drug prevalence targets were not achieved and the 2006/07 drug prevalence survey reported increases in recent and current use. The target of having substance use policies in all schools was near completion at the time of a Department of Education and Science survey in 2005. A number of data sources were used to estimate the levels of early school leaving and, while precise figures were not available, it appeared that early school leaving had decreased during the period of the NDS 2001–2008.
While many of the actions relating to the implementation of prevention programmes were completed or near completion, the Steering Group questions the effectiveness of a number of the programmes. Despite the high number of schools which reported that they had implemented substance misuse policies, the quality of these policies had not been assessed and there was a need to determine how actively they were being implemented. The Social Personal Health Education (SPHE) programme, the foundation for developing awareness of drugs and alcohol issues in schools, is a mandatory part of the curriculum but its effectiveness as a drug prevention measure was consistently questioned during the consultation process.
Treatment and rehabilitation
Three of the KPIs under this pillar specified increased availability of treatment and harm reduction services, and one sought a reduction in the incidence of HIV. The target of a maximum waiting period of one month for treatment for problem drug use was achieved for almost all non-opiate addiction cases. However, there were still difficulties in many areas in providing access to methadone treatment within one month of assessment. No under-18s had had to wait longer than one month to initiate treatment following assessment, but there were still not enough residential places or community supports. There was limited progress in providing harm-reduction services, but the incidence of HIV among injecting drug users had seen a consistent reduction. The incidence of hepatitis C continued to cause concern.
While rehabilitation was covered under the treatment pillar in the NDS 2001–2008, the mid-term review (MTR) of the strategy recommended that a separate pillar be established.7 Following a recommendation in the report of the Working Group on drugs rehabilitation,8 a National Drug Rehabilitation Implementation Committee (NDRIC), chaired by the HSE, was set up. The Steering Group notes that there was progress in several areas related to the MTR’s recommendation to strengthen support for families, and that the HSE had significantly developed its family support services.
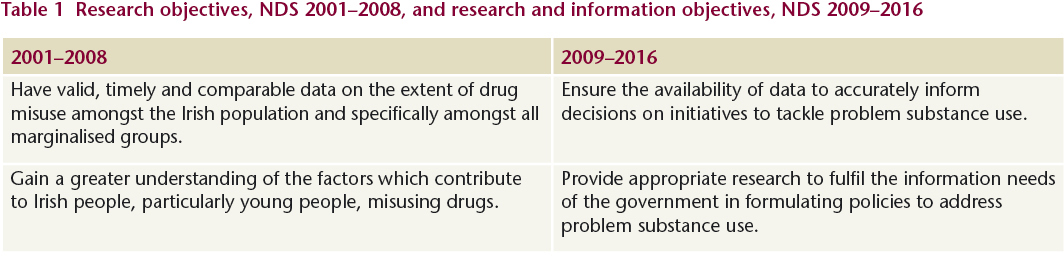
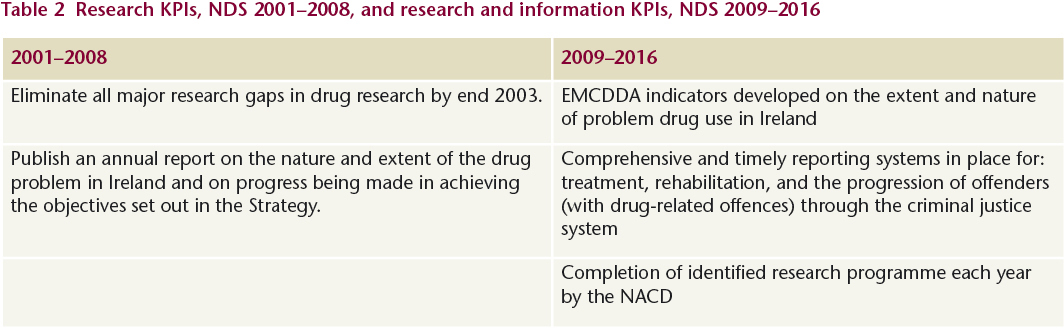
Research
The KPIs under this pillar dealt with information on prevalence in the general population, problem drug use, demand for drug treatment, drug-related deaths and drug-related infectious diseases. In 2005 the NACD published the findings of a drug prevalence survey carried out in Ireland and Northern Ireland in 2002/03. This survey was repeated in 2006/07 and the results published in 2008. The NACD also commissioned studies on drug prevalence among vulnerable groups, including the homeless, new communities in Ireland and Travellers. Other studies give some insight into alcohol and cannabis use among the youth and school-going populations. While work on the second 3-source capture-recapture study to estimate the prevalence of problematic opiate use has yet to be completed, the Research Outcome Study in Ireland (ROSIE) and the information reported by the NDTRS provide significant insights into the patterns of problem drug use.
Improvements in the reporting of problem drug use to the Drug Misuse Research Division (renamed Alcohol and Drug Research Unit (ADRU) in 2007) increased the efficiency of the flow of this data and the quality of the information. The ADRU manages the National Drug Treatment Reporting System (NDTRS). This system collects data on episodes of treatment, rather than on the individual person treated; neither does it provide outcome/exit data for all areas. In 2005 the Health Research Board (HRB) developed a National Drug-Related Deaths Index (NDRDI), which subsequently published data for the period 1998–2005.2 The Health Protection Surveillance Centre (HPSC) introduced an extended surveillance system for hepatitis B in 2004 and for hepatitis C in 2007. The Steering Group notes that there has been no concerted effort to monitor the incidence and prevalence of hepatitis B, hepatitis C or HIV among drug users since the NDS 2001–2008 was launched.
Inclusion of alcohol in new substance misuse strategy
Announcing the decision to develop a ‘substance misuse’ strategy, including both illicit drugs and alcohol, Minister of State with responsibility for drugs strategy, John Curran TD, said: ‘A combined strategy will facilitate a more coherent approach to the issues and consequences of alcohol and illicit drug use including addictive behaviours. We cannot continue to look at these problems in isolation.’9 A new steering group will be established in autumn 2009 to develop proposals for a strategy that will incorporate the already-agreed drugs policy element. Membership of the new steering group will reflect the appropriate statutory, community/voluntary and other relevant interests. The group will be jointly chaired by officials from the Department of Health and Children and the Office of the Minister for Drugs and will be asked to report by the end of 2010.
The interim drugs strategy contains a number of proposals relating to alcohol. These are summarised below.
Supply reduction
During the public consultation process, the issue of underage drinking was consistently raised, both as a problem in its own right and as a gateway to the use of illicit drugs. However, owing to the fundamental legal difference involved in their supply, the focus in the interim drugs strategy is on illicit drugs rather than on alcohol, with the exception of underage drinking.
Prevention
Alcohol is referenced under this pillar with regard to developing a prevention strategy to tackle substance misuse, particularly in relation to under-18s. One of the key themes to emerge from the consultation process was the perception that drug and alcohol use are becoming more widespread and that the age profile of those involved is getting younger. Measures to prevent and/or delay drug and alcohol use – especially among young people – are, therefore, particularly important and urgent.
The Steering Group is of the view that renewed efforts need to be made to address the issue ofunderage drinking, which is often perceived as the direct, or underlying, cause of many of the problems encountered by individuals and communities. The Group acknowledges the benefits of the enactment of the Intoxicating Liquor Act 2008. However, it also feels that the impact of the legislative measures, and the situation generally, should be monitored to ensure that alcohol is not being supplied to under-18-year-olds in an illegal or irresponsible way.
Alcohol advertising and sponsorship (especially in the sporting context) are seen as particular problems, especially as the messages often target the young and impressionable. The Department of Health and Children established a working group to engage with relevant stakeholders and sporting bodies to examine the extent of sports sponsorship by alcohol companies and to consider how the health-related concerns might be addressed. The working group is expected to report in autumn 2009. The Steering Group welcomes these developments.
Provision of recreational and other facilities for young people is considered to be important in preventing misuse of drugs and alcohol, and the Steering Group identifies the lack of such facilities and appropriate supporting structures across the country as a key gap. The Group believes that access to school facilities outside school hours should be progressed as a matter of urgency.
The Steering Group is of the view that there is a need to further develop and promote prevention strategies in a number of other key areas – third-level institutions, workplaces, sports and other community and voluntary organisations – using brief interventions where appropriate.
The development of a tiered or graduated approach to prevention and education measures in relation to drugs and alcohol is recommended. This approach would provide a framework for the future design of targeted prevention and education interventions.
Treatment and rehabilitation
The Steering Group endorses the view of the Working Group on Alcohol and Drug Synergies that greater coherence and co-ordination of alcohol and drug issues at policy, planning and operational levels are needed. With respect to treatment and rehabilitation, the Steering Group sees the re-orientation of all addiction services towards dealing with problem substance use as a key feature of the new strategy.
The Steering Group acknowledges that it is not possible to quantify the number of problem alcohol users requiring treatment. However, the significant difference between the number of alcohol-related hospital discharges and the number of reported cases receiving treatment for alcohol addiction indicates that there is a considerable cohort of problem alcohol users who could benefit from engagement with addiction treatment services.
The Steering Group believes that training in brief interventions needs to be rolled out across the healthcare service to maximise the impact of this cost-effective approach. Early interventions, targeted at hazardous and harmful users of alcohol, are designed to reduce alcohol consumption before dependence develops. There is strong evidence to suggest that brief interventions provided within various healthcare settings, including primary care, general hospital wards, mental health services and emergency departments, are effective in reducing hazardous and harmful alcohol use.
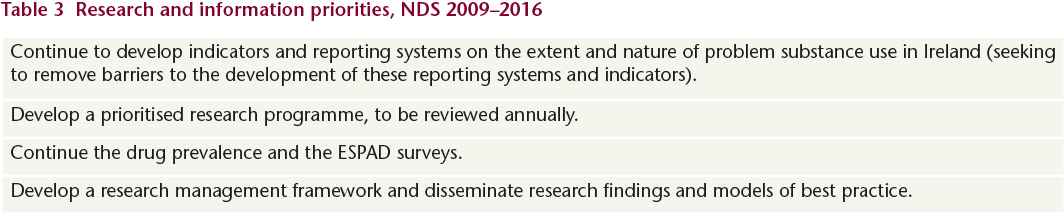
Research and information
The Steering Group recommends the development of a research management framework in relation to problem substance use in Ireland. In relation to alcohol, it specifically recommends:
· the development of appropriate epidemiological indicators of problem alcohol use, and building on existing monitoring systems and prevalence surveys;
· measuring the impact of alcohol and drugs on the Irish health and justice systems; and
· monitoring problem substance use (including alcohol) among those presenting to hospital emergency departments.
(Johnny Connolly, Brian Galvin, Martin Keane, Jean Long, Suzi Lyons, Deirdre Mongan and Brigid Pike)
1. Department of Community, Rural and Gaeltacht Affairs (2009) National Drugs Strategy (interim) 2009–2016. Dublin: Stationery Office.
2. Lyons S, Lynn E, Walsh S and Long J (2008) Trends in drug-related deaths and deaths among drug users in Ireland, 1998–2005. HRB Trends Series 4. Dublin: Health Research Board.
3. Organisation for Economic Co-operation and Development (2008) Ireland: towards an integrated public service. Paris: OECD.
4. Whelan P, Arnold T, Aylward A, Doyle M, Lacey B, Loftus C, McLoughlin N, Molloy E, Payne J and Pine M (2003) Cross-departmental challenges: a whole-of-government approach for the twenty-first century. Dublin: Institute of Public Administration.
5. Pike B (2008) Development of Ireland’s drug strategy 2000–2007. HRB Overview Series 8. Dublin: Health Research Board.
6. The KPIs used to measure progress under the pillars in the NDS 2001–2008 were revised by the Steering Group that undertook the mid-term review of the drugs strategy.
7. Steering Group for the mid-term review of the National Drugs Strategy (2005) Mid-term review of the National Drugs Strategy 2001–2008. Dublin: Department of Community, Rural and Gaeltacht Affairs.
8. Working group on drugs rehabilitation (2007) National Drugs Strategy 2001–2008: rehabilitation. Dublin: Department of Community, Rural and Gaeltacht Affairs.
9. Curran J (2009) Alcohol and drugs to be joined in a National Substance Misuse Strategy. Press release issued 31 March 2009 by the Department of Community, Rural and Gaeltacht Affairs.