Long, Jean (2004) Updated analysis from the National Drug Treatment Reporting System. Drugnet Ireland, Issue 12, December 2004, pp. 22-24.
| Preview | Title | Contact |
|---|---|---|
|
PDF (Drugnet Ireland, issue 12)
- Published Version
263kB |
Between June and September 2004, staff at the DMRD published three occasional papers on treated drug misuse in the seven health board areas outside the Eastern Regional Health Authority (ERHA) area, namely:the Midland, Mid-Western, North Eastern, North Western, Southern, South Eastern and Western Health Boards. The analysis presented in these papers is based on data submitted by service providers to the National Drug Treatment Reporting System (NDTRS).
Occasional Paper 11: Treatment demand in the seven health boards areas outside the ERHA, 1998 to 2002
The data presented in Occasional Paper 11 provide a description of demand for drug treatment services in seven health boards. This paper will help inform service planning and provision.
The main findings and their implications are:
· The number of new and previously treated cases in the seven health boards (outside the ERHA area) almost trebled between 1998 and 2002.
· Both new and previously treated cases in the seven health board areas most frequently reported that cannabis was their main problem drug between 1998 and 2002. The total number of cases reporting cannabis as their main problem drug trebled, increasing from 409 in 1998 to 1,359 in 2002. The numbers reporting problem opiate use almost trebled, from 184 in 1998 to 532 in 2002. Opiate use was more common in the health board areas bordering the ERHA area. Though small, the numbers reporting cocaine use increased consistently. The wide spectrum of problem drugs reported indicates that treatment services need to cater for a number of licit and illicit drugs used rather than focusing on one or two drugs.
· Although there was a small decrease in the proportion of cases taking more than one drug (polydrug use), from 84 per cent in 1998 to 77 per cent in 2002, it remained a common practice and is associated with poorer treatment outcomes. Polydrug use is an issue that needs to be addressed in a client’s treatment plan.
· The number of cases who reported injecting more than doubled, from 148 in 1998 to 342 in 2002. Half of the injector cases had started injecting before they were 20 years old. Injectors have a higher risk of acquiring blood-borne viral infections and experiencing overdose than non-injectors. This suggests that the drug treatment services outside the ERHA area require prevention and treatment interventions to deal with blood-borne viruses (in particular HIV, hepatitis B, and hepatitis C) and drug overdose (in particular opiate-related overdose).
· The proportion of cases under 18 years old increased by four per cent over the reporting period and, as expected, was much higher for new cases than for those previously treated. Those under 18 years old require different approaches to treatment and it is important that this is recognised in service planning.
· The low levels of educational achievement and employment among chronic problem drug users emphasises the importance of close links between treatment interventions and social and occupational reintegration programmes.
Occasional Paper 12: Trends in treated problem drug use in the seven health boards areas outside the ERHA, 1998 to 2002
The data presented in this paper describe trends in treated problem drug use in seven health board areas. The total numbers include 7,545 cases who lived and were treated in the seven health boards between 1998 and 2002. In this paper, problem drug use is described in relation to person, place and time. This paper will assist policy makers, service planners and public health practitioners to develop appropriate responses to problem drug use in the future.
The main findings and their implications are:
- Both the incidence and prevalence of treated problem drug use almost trebled between 1998 and 2002 (Figure 1). For example, the incidence of treated problem drug use increased from 24.8 per 100,000 of the population in 1998 to 69.7 per 100,000 in 2002. This observed increase may be explained by a true increase in use, an increase in access to treatment services, new legislation encouraging more people into treatment, or an increase in the number of centres reporting cases to the NDTRS. The most likely explanation is a combination of all these factors.
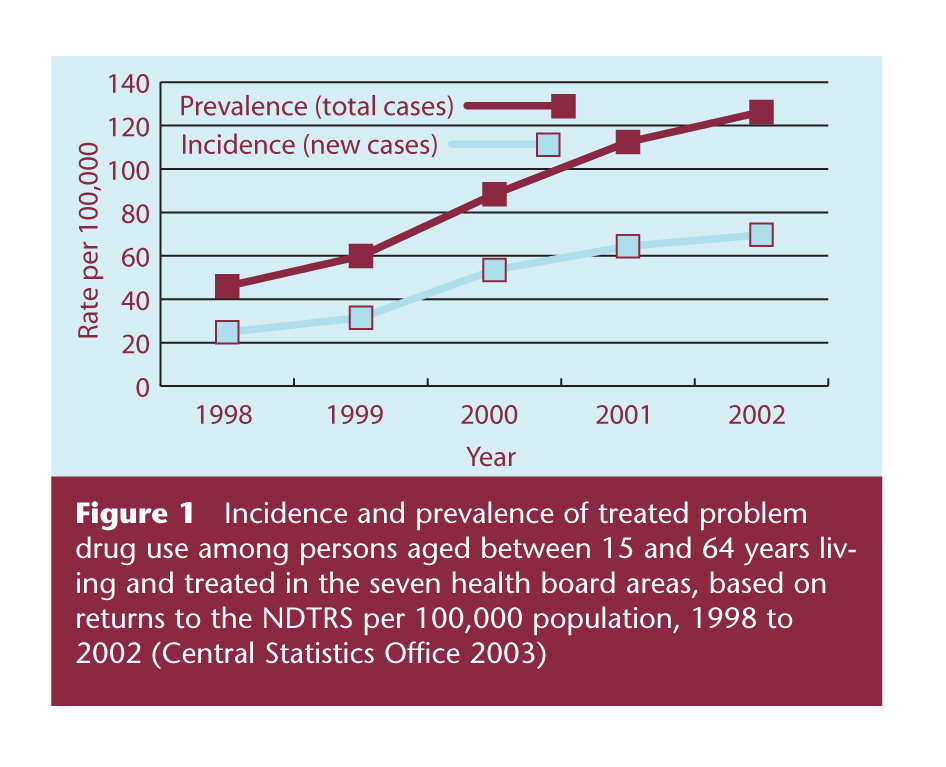
Figure 1 Incidence and prevalence of treated problem drug use among persons aged between 15 and 64 years living and treated in the seven health board areas, based on returns to the NDTRS per 100,000 population, 1998 to 2002 (Central Statistics Office 2003 )
- The incidence of treated problem drug use for the reporting period was highest in the Southern Health Board area, followed closely by the South Eastern Health Board area. The Western Health Board area had the lowest incidence, indicating lower drug use rates than in the rest of Ireland, lower access to or uptake of appropriate treatment services, or lower levels of participation in the NDTRS. This requires investigation.
- The total number of cases reporting cannabis as their main problem drug trebled, increasing from 392 in 1998 to 1,328 in 2002. The numbers reporting problem opiate use also increased steadily, from 116 in 1998 to 439 in 2002. Opiate use was more common in the health board areas bordering the ERHA area. The second most frequently reported main problem drug was ecstasy for new cases and opiates for previously treated cases. Though small, the number of new cases reporting cocaine use increased from six in 1998 to 42 in 2002. These findings indicate that treatment services must cater for a wide spectrum of illicit drugs rather than focus on one or two drugs, and must be capable of adjusting treatment approaches in accordance with changing patterns of problem drug use.
- Although there was a small percentage decrease in polydrug use, from 84 per cent of cases in 1998 to 79 per cent in 2002, it remained a common practice and is associated with poorer treatment outcomes.
- The number of cases who reported injecting trebled, increasing from 96 in 1998 to 284 in 2002. Injectors have a higher risk of acquiring blood-borne viral infections and experiencing overdose than non-injectors.
- The proportion of cases under 18 years old increased by just over three per cent during the reporting period and, as expected, was much higher for new cases than for those previously treated. Those under 18 years old require different approaches to treatment and it is important that this is a consideration during service planning.
- The main problem drug reported by new cases was examined by selected socio-demographic and drug-using characteristics and some important relationships were identified. Young teenagers initiated drug use with cannabis and volatile inhalants. The use of opiates, ecstasy and amphetamines was commenced in mid to late teens. There were differences in type of drug used by males and females, with very high proportions of males treated for cocaine and cannabis use compared to their female counterparts. The highest rates of employment were among those using drugs commonly associated with social events, and the lowest rates of employment were among those who used opiates and benzodiazepines. This observation (along with the high rates of early school leaving) has important implications for the social and occupational reintegration of opiate and benzodiazepine users.
Occasional Paper 13: Trends in treated problem opiate use in the seven health board areas outside the ERHA, 1998 to 2002
The data presented in this paper describe trends in treated problem opiate use in seven health board areas. The total numbers include the 1,495 opiate cases who lived and were treated in the seven health board areas between 1998 and 2002. In this paper, treated problem opiate use is described in relation to person, place and time. This paper will assist policy makers, service planners and practitioners to develop appropriate responses to problem opiate use in the seven health board areas.
The main findings and their implications are:
- The incidence of treated problem opiate use increased sharply, from 2.0 in 1998 to 8.3 in 2002, per 100,000 of the 15–64-year-old population (Figure 2). The increase in new problem opiate users at treatment services indicates a spread of heroin use in the seven health board areas.
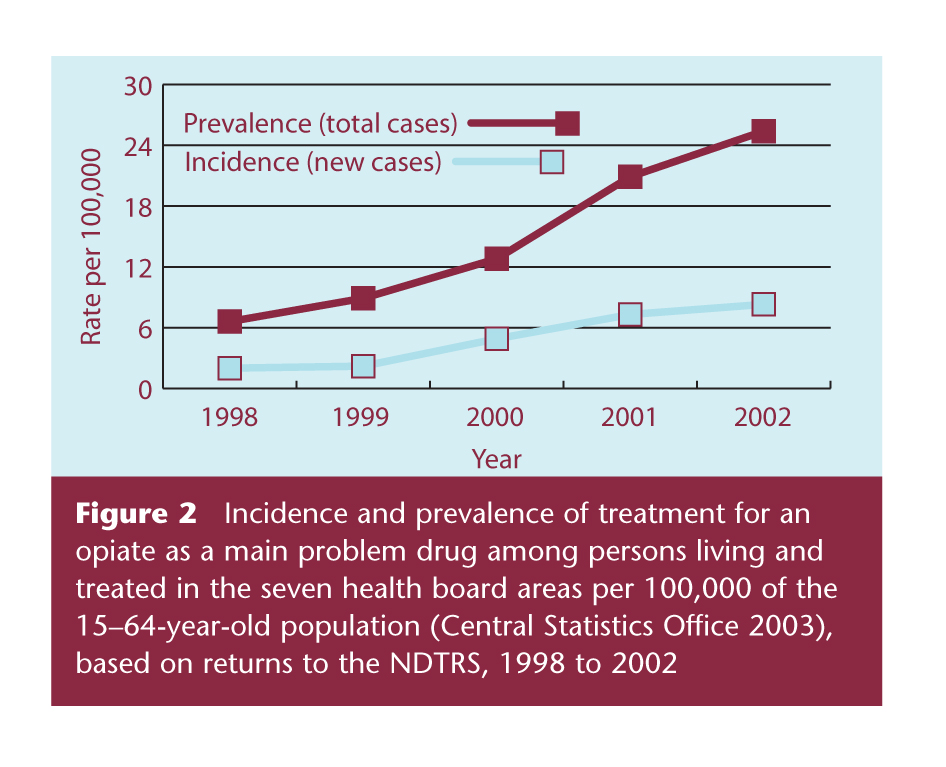
Figure 2 Incidence and prevalence of treatment for an opiate as a main problem drug among persons living and treated in the seven health board areas per 100,000 of the 15–64-year-old population (Central Statistics Office 2003), based on returns to the NDTRS, 1998 to 2002
- The prevalence of treated problem opiate use has also increased steadily, from 6.6 per 100,000 of the 15–64-year-old population in 1998 to 25.4 in 2002, and this is an indicator that problem heroin use has a chronic element requiring continued care or repeated treatment over time.
- There was a spread by county in demand for treatment for problem opiate use among new cases living in the seven health board areas, with very high rates of treated problem opiate use in counties Carlow, Cavan, Louth, Meath, and Westmeath. These data will be useful when assessing the adequacy of existing services or identifying new sites for treatment services.
- The lowest rates of treatment for problem opiate use were along the western seaboard; this may be partly due to under-reporting.
- For new cases reporting problem opiate use, the time interval between commencing opiate use and starting treatment remained between 3.5 and 3.8 years from 1999 to 2002. Polydrug-using practices may be initiated during the interval between first taking any drug and the age at which opiate treatment is sought. During the time interval between commencing opiate use and seeking treatment, opiate users may change from smoking to injecting opiates and, subsequently, may contract blood-borne viruses, such as hepatitis C, indicating the need for proactive interventions to discourage the move from smoking to injecting and bring opiate users into treatment earlier.
- The proportion of opiate cases treated in the seven health board areas who reported polydrug use decreased from 80 per cent in 1998 to 74 per cent in 2002. Polydrug use is one of the factors that may impede successful treatment for problem opiate use unless specific interventions are introduced to address this problem.
- For cases treated in the seven health board areas who reported opiates as their main problem drug and reported using more than one drug, the most common secondary drug used was cannabis. During the period under review, the use of cocaine and benzodiazepines as second drugs increased, while the use of amphetamines as a second drug decreased. An exact knowledge of polydrug use is very important for the correct and comprehensive management of opiate users.
- Of note, there was an increase in the actual number of injectors in the seven health board areas. Opiate injectors have a higher risk of acquiring blood-borne viral infections and of experiencing overdose than non-injectors. This suggests that the incidence of blood-borne viral infections and opiate-related deaths has increased in the seven health board areas during the period under review, but specific data are not available.
- Problem opiate users’ educational characteristics indicate that individuals who leave school early are more likely to become problem opiate users, or that the lifestyle of problem opiate users renders it difficult to stay in full time education, or a combination of both factors. In line with national employment trends, there was an increase in the proportion of new and previously treated opiate cases who reported having regular employment up to 2001 and a subsequent decrease in 2002. Taken together, these two findings indicate the importance of a social, educational and economic reintegration strategy for the successful treatment of opiate users.
Long J, Kelleher T, Kelly F, Sinclair H (2004) Treatment demand in the seven health boards outside the ERHA, 1998 to 2002. Occasional Paper 11. Dublin: Health Research Board.
Long J, Kelleher T, Kelly F, Sinclair H (2004) Trends in treated problem drug use in the seven health boards outside the ERHA, 1998 to 2002. Occasional Paper 12. Dublin: Health Research Board.
Long J, Kelleher T, Kelly F, Sinclair H (2004) Trends in treated problem opiate use in the seven health boards outside the ERHA, 1998 to 2002. Occasional Paper 13. Dublin: Health Research Board.
These papers are available on the Health Research Board website at http://www.hrb.ie
Repository Staff Only: item control page