Keane, Martin
(2012)
CRA, ACRA and CRAFT: a brief review of the evidence.
Drugnet Ireland,
Issue 41, Spring 2012,
pp. 16-17.
The Community Reinforcement Approach (CRA) is acknowledged in the National Drugs Strategy as an effective evidence-based approach that could be used as an adjunctive to services delivered within the rehabilitation pillar.
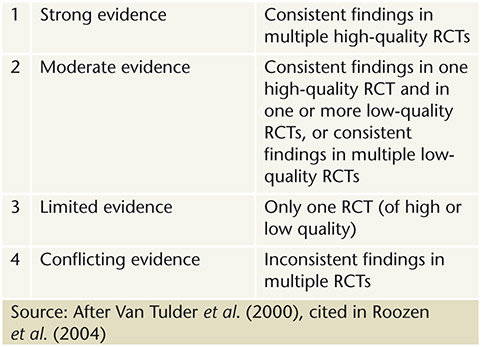
Roozen et al. (2004) undertook a meta-analysis of 11 randomised controlled trials (RCTs) to review the effectiveness of two approaches to treating substance abuse: (i) Community Reinforcement Approach (CRA) versus usual care, and (ii) CRA versus CRA with contingency management. A qualitative analysis was also performed using a four-level rating system (Table 1).
The authors report that there is strong evidence that CRA is more effective than usual care in reducing the number of days alcohol is consumed, and conflicting evidence on its effectiveness in maintaining continued abstinence. There is moderate evidence that CRA with disulfiram (Antabuse) is more effective than usual care with disulfiram in reducing the number of days alcohol is consumed, and limited evidence for no difference in effect between CRA with disulfiram and usual care with disulfiram on continuing abstinence.
There is strong evidence that CRA with ‘incentives’ is more effective than usual care in achieving abstinence from cocaine use. There is strong evidence that CRA with abstinent-contingent incentives is more effective than CRA without abstinent-contingent incentives in achieving abstinence from cocaine use.
There is limited evidence that CRA with incentives is more effective than usual care in an opioid detox programme and there is limited evidence that CRA on its own is more effective than usual care in achieving abstinence through a methadone maintenance programme.
The review by Roozen and colleagues represents the most rigorous analysis of the evidence base on CRA; however, it only covers studies undertaken before 2004. No high-quality analysis has been located since then. The review is useful as it examines the effectiveness of CRA in tackling the use and misuse of different substances, both when used alone and in combination with medications and contingency management incentives. This type of review is a useful source of information to a diverse body of practitioners working in the substance misuse field. Regarding the strength of the evidence base for CRA (pre-2004), the authors state: ‘In general, there is limited to moderate evidence for the efficacy of CRA with or without medication or contingency management in various substance-related disorders, including alcohol, cocaine and heroin.’
Abbot (2009) reviewed published research on the use of CRA in the treatment of opioid dependence. The review included three randomised and one non-randomised controlled trials. The review is different from that of Roozen et al. in that Abbot summarises the findings from the four trials whereas Roozen and colleagues synthesise the findings from 11 trials to compute a new and overall estimate of effectiveness.
Abbott concludes that CRA, when combined with methadone reduces opioid use and use of other drugs and, in one study, improved legal status, reduced psychiatric symptoms and improved social and vocational functioning. When combined with vouchers (contingency management), CRA can retain people in treatment long enough to achieve detoxification from buprenorphine.
In a study undertaken in a less clinical setting than previous studies, Slesnick et al. (2007) randomly assigned 96 homeless young people aged 14-22 to a CRA and 84 homeless youth to treatment as usual (TAU) at a homeless drop-in centre in the US. Homeless youth assigned to CRA showed greater improvement in respect of substance use, social stability and depression from baseline to six months compared to those assigned to TAU. However, those receiving TAU also showed improvement in several domains. Acknowledging the design limitations of the trial and the need for caution when drawing conclusions from these outcomes, the authors note that ‘the research design is limited in that youth were only assessed at post-treatment. A longer follow-up is needed to determine stability of treatment effects.’
Smith et al. (2008) describes the CRAFT programme as an outgrowth of the CRA. The CRAFT programme works with concerned family members to rearrange contingencies in the alcohol abuser’s environment so that alcohol abuse in discouraged and sobriety is encouraged. The ultimate goal of the CRAFT programme is to equip concerned family members with the skills to influence the alcohol abuser to engage with treatment. Smith and colleagues provide a brief review of a number of both randomised and non-randomised studies that evaluated the effectiveness of CRAFT in comparison with Al-Anon and other interventions. Most of the studies showed that CRAFT was more effective in helping concerned family members to persuade the substance abusers to engage with treatment. However, the data provided are much too brief to enable a rigorous critical appraisal of the studies.
An additional recent outgrowth of the CRA is the Adolescent Community Reinforcement Approach (ACRA), which aims to make an alcohol- and drug-free lifestyle more rewarding than continued substance abuse. In a recent study that compared the outcomes of 151 adolescents (aged under 18) and 152 emerging adults (aged 18–25), who were diagnosed with substance misuse disorders and had received the ACRA programme, Douglas et al. (2011) found that emerging adults were less likely to be abstinent and had more days of alcohol use compared to adolescents after both received the ACRA programme.
Abbott PJ (2009) A review of the Community Reinforcement Approach in the treatment of opioid dependence. Journal of Psychoactive Drugs, 41(4): 379–385.
Meyers RJ, Villanueva M and Smith JE (2005) The Community Reinforcement Approach: history and new directions. Journal of Cognitive Psychotherapy, 19(3): 251–264.
Roozen HG, Boulogne JJ, van Tulder MW, van den Brink W, De Jong CA and Kerkhof AJ (2004) A systematic review of the effectiveness of the community reinforcement approach in alcohol, cocaine and opioid addiction. Drug and Alcohol Dependence, 74(1): 1–13.
Slesnick N, Prestopnik J, Meyers RJ and Glassman M (2007) Treatment outcomes for street-living, homeless youth. Addictive Behaviours, 32(6): 1237–1251.
Smith JE, Meyers RJ and Austin JL (2008) Working with family members to engage treatment-refusing drinkers. Alcoholism Treatment Quarterly, 26(1/2): 169–193.
![[img]](https://www.drugsandalcohol.ie/style/images/fileicons/application_pdf.png)