Lyons, Suzi (2014) European research on risk factors for overdose. Drugnet Ireland, Issue 49, Spring 2014, pp. 11-13.
| Preview | Title | Contact |
|---|---|---|
![[img]](https://www.drugsandalcohol.ie/style/images/fileicons/application_pdf.png) |
PDF (Drugnet Ireland 49)
- Published Version
1MB |
Opiates (both illicit and prescribed) continue to be a significant factor in many poisoning deaths, not only in this country (see article on p. x) but also internationally. In international literature, poisonings are also known as drug-induced deaths or overdose. Some of the key findings about opiate overdose in Europe are shown in the box
· There are 1.4 million problem opiate users in Europe.
· There were 6,500 overdose deaths in 2011.
· There were more than 70,000 overdose deaths during the first decade of the 21st century.
· Overdose deaths represent 4% of all deaths in adult males aged under 40.
· Half of all deaths in people who regularly inject heroin are attributable to overdose.
· On average, heroin users who overdose report having experienced three overdoses.
· Many heroin users who survived an overdose did not perceive themselves to be at high risk of overdose, even though they had a history of overdose in the previous six months.
Sources: EMCDDA (2013)1 and Frisher et al. (2012)2
Several recent publications have looked at the risk factors for overdose and strategies for prevention.1,2,3
Risk factors
There are many, often inter-related, risk factors for fatal and non-fatal overdose. Recognition of these factors can help prevent the occurrence of overdose. Availability of opiates, route of administration, polydrug use, periods of abstinence and health of the user are some of the common factors.2,3 Based on a comprehensive review of the literature, Frischer et al. (2012) identified and classified risk factors at three levels: individual, observers and organisational. The table below lists the individual risk factors. Observer risk factors relate to the perceived consequences of becoming involved, e.g. risk of arrest if police are called. Organisational risk factors relate to the availability and flexibility of the treatment, response to treatment and misuse of prescription drugs. Another resource in this area is the ORION Project.4 This is an ehealth tool for assessing overdose risks factors and is available for download from http://orion-euproject.com.
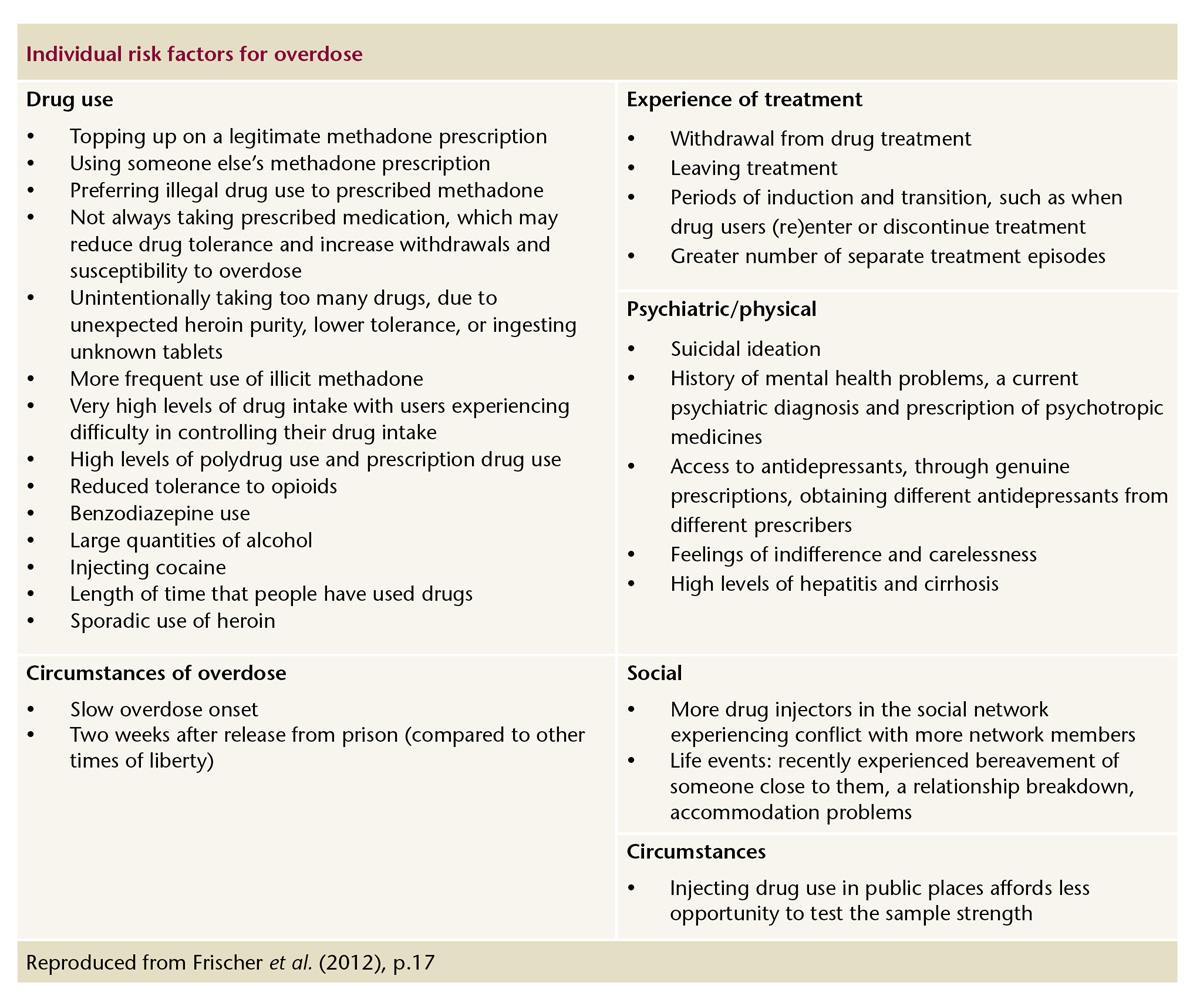
Reproduced from Frischer et al. (2012), p.17
The literature points to several main areas for prevention, both to reduce the risk of an overdose occurring and to prevent fatality in the event of an overdose.
Overdose prevention information and training
The literature shows that problem opiate users often underestimate their risk of overdose1 so information, counselling and training to recognise the risks for, and signs of, overdose is vital. This information, along with training in basic cardio-pulmonary resuscitation, should also be provided to family and friends.
Treatment
Access to, and retention in, treatment, including opiate substitution treatment, is one of the best ways to reduce opiate-related deaths.1,2,3
Co-ordinated release from prison
The increased risk of death from overdose in the first weeks after release from prison is well documented.5
Strategies to reduce this risk include increasing the availability of drug treatment in prison, pre-release counselling and overdose prevention information, co-ordination with the community to ensure continuity of treatment, and availability of social supports on release.
Reducing the availability of opiates
The United Nations Office on Drugs and Crime (UNODC) notes the rise in the number of overdose deaths owing to prescription opiates, particularly in the US.3 It recommends specific strategies, including real-time monitoring of the prescription of opiates, reduced prescribing, and promoting greater awareness among health professionals of the risks of long-term prescribing for chronic conditions.
Preventing fatalities in the event of an overdose
Take-home naloxone is already available in five European countries as part of their overdose prevention strategies (see article on p.13). Of note, the most recent figures from the National Drug-Related Deaths Index (NDRDI) show that 59% of all poisoning deaths in Ireland in 2011 involved more than one drug, in many cases a benzodiazepine along with one or more other substances.6 Naloxone is only effective in reversing opiate overdose and therefore a range of strategies is needed to prevent overdose deaths when polydrug use is prevalent.
Another prevention strategy is to improve bystander response by providing information and training to enable those on the scene to recognise and respond to the overdose. Naloxone can be administered by bystanders (family, friends or other drug users) if they are properly trained.
The EMCDDA cites the availability of supervised drug consumption rooms which are targeted at a very specific group of users as another strategy to reduce fatalities in the event of overdose.3 Seven European countries have such facilities. They are usually integrated into a service which offers a range of other harm reduction, medical and social services.
Conclusion
The issues involved in preventing overdose are summarised by Frisher et al. (2012):
[T]here is evidence that many interventions may reduce overdose, particularly in settings where the drug user is in contact with treatment or emergency services. However, it is important to bear in mind the distinction between overdose prevention at the clinical and at the population level. At the clinical level, specific interventions are available and have been shown to be effective (e.g. pharmacological treatment). At the population level, where many drug users are not in contact with services, overdose reduction depends on behavioural change by drug users themselves (e.g. avoiding the mixture of opiates and other depressant drugs). Overdose prevention is a multifaceted problem. Purely technological interventions were thought likely to have a relatively limited impact. Rather, overdose involves personal and societal issues; only when these are addressed is the level of fatal overdose in Europe likely to decrease. (pp. 4–5)
1. European Monitoring Centre for Drugs and Drug Addiction (2013) Perspectives on drugs: preventing overdose deaths in Europe. Lisbon: EMCDDA. http://www.emcdda.europa.eu/topics/pods/preventing-overdose-deaths
2. Frisher M, Baldacchino A, Crome I and Bloor R (2012) Preventing opioid overdoses in Europe: a critical assessment of known risk factors and preventative measures. Lisbon: EMCDDA. www.drugsandalcohol.ie/18701
3. UNODC and WHO (2013) Opioid overdose: preventing and reducing opioid overdose mortality. Discussion paper.Vienna: United Nations. www.drugsandalcohol.ie/20068
4. Lynn E (2014) The overdose risk information (ORION) project. Drugnet Ireland, (48): 14. www.drugsandalcohol.ie/21212
5. Lyons S, Walsh S, Lynn E and Long J (2010) Drug-related deaths among recently released prisoners in Ireland, 1998 to 2005. International Journal of Prisoner Health, 6(1): 26–32. www.drugsandalcohol.ie/13332
6. Health Research Board (2014) Drug-related deaths and deaths among drug users in Ireland: 2011 figures from the National Drug-Related Deaths Index. www.drugsandalcohol.ie/21005
Item Type
Article
Issue Title
Issue 49, Spring 2014
Date
April 2014
Page Range
pp. 11-13
Publisher
Health Research Board
Volume
Issue 49, Spring 2014
EndNote
Accession Number
HRB (Electronic Only)
Repository Staff Only: item control page